


Cards In This Set
| Front | Back |
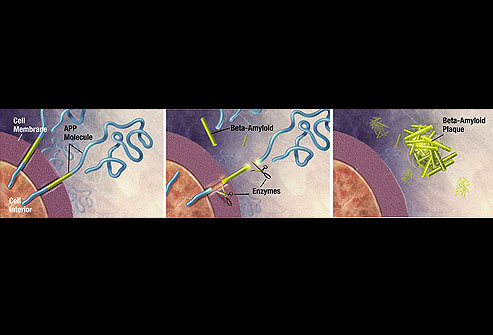 Pathogenesis of AD |
Amyloid, or senile, plaques are dense, insoluble deposits of
amyloid-beta proteins, which are fragments of amyloid precursor proteins
(APP), a transmembrane neuronal protein. As these proteins are
enzymatically broken down, they clump together, forming the dense
structures identifiable as amyloid plaques. These plaques primarily
accumulate in the association cortices and hippocampus.
|
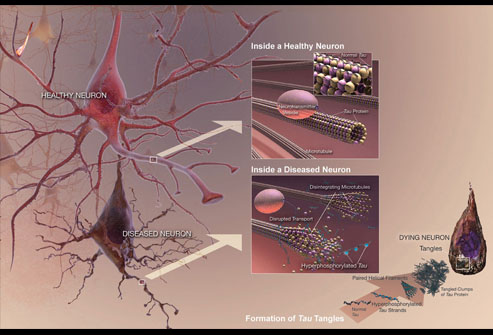 Pathogenesis of AD |
Neurofibrillary tangles develop when microtubule tau proteins become
hyperphosphorylated and aggregate within the neuronal cells. These
tangles break down the neurons' ability to transport molecules along the
axon. Neurofibrillary tangles initially form in the medial aspect and
pole of the temporal lobe, especially the hippocampus. With increasing
disease progression, they spread throughout the cortex, beginning in the
high-order association regions and less commonly in the primary motor
and sensory regions.
|
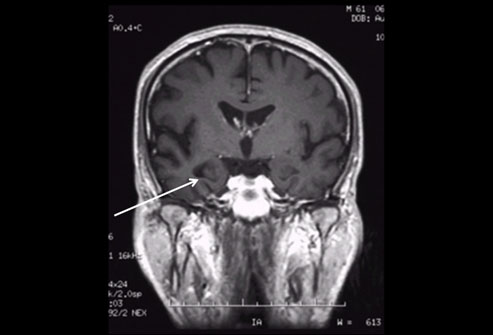 Brain image |
Neuroimaging provides an excellent means of grossly examining the brain.
It allows for volumetric measurements of individual structures and can
be repeated over time as a coarse means of measuring disease
progression. Neuroimaging also allows for exclusion of many reversible
causes of dementia. Magnetic resonance imaging (MRI) is the preferred
modality of imaging because it allows for excellent 3-dimensional
visualization, especially of the hippocampus. The most common findings
are cortical atrophy, dilated ventricles, and accentuated cortical
sulci. On the T1-weighted MRI shown, extensive hippocampal atrophy has
occurred on the right side (see arrow).
|
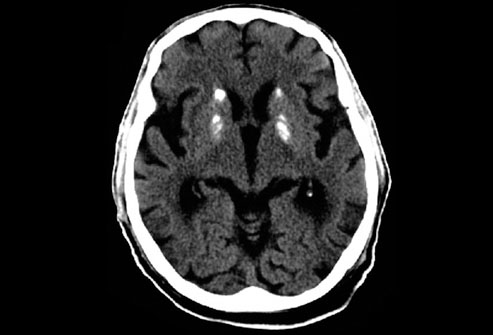 Ct scan |
Computed tomography (CT) is not as useful as MRI in diagnosing or
following the progression of Alzheimer's disease, although it is
commonly used as a first-line modality in patients who present with
dementia. The principal findings are similar in both modalities and
changes over time are useful; however, on a CT scan, the etiology of
cerebral atrophy is more difficult to discriminate between Alzheimer's
disease and normal aging. The CT scan shown here demonstrates several
areas of calcification within the basal ganglia, the result of extreme degeneration in a patient with Down's syndrome and early Alzheimer's disease
|
 Treatment of AD |
Current treatment regimens for Alzheimer's disease focus on symptomatic
therapy, as no proven disease-modifying therapies exist. The standard
medications are cholinesterase inhibitors (ChEIs) and partial N-methyl-D-aspartate
(NMDA) antagonists. ChEIs act by preventing the breakdown of
acetylcholine, because cholinergic systems that modulate information
processing are thought to be impaired. Partial NMDA antagonists are
thought to improve the signal-to-noise ratio of glutamatergic
transmission. Both classes of medication may be used together and
provide modest symptomatic improvement but do nothing to prevent disease
progression. Frequently, psychotropic medications are also included to
treat the secondary symptoms (eg, depression, agitation, sleep
disorders) that develop. Image included with permission and copyrighted
by First DataBank, Inc.
|
